All India Radio

Enhancing the Health Infrastructure of the Country
Search 12th February, 2019 Spotlight here: http://www.newsonair.com/Main_Audio_Bulletins_Search.aspx
TOPIC: General Studies 2
- Issues relating to development and management of Social Sector/Services relating to Health, Education, Human Resources
- Government policies and interventions for development in various sectors and issues arising out of their design and implementation.
In News: There is an increase of more than Rs 7,000 crore in nominal terms from last year’s expenditure on health in this year’s budget — the outlay has increased from Rs 56,045 crore to Rs 63,298 crore. Accounting for inflation, this amounts to a 9.2 per cent increase in real terms.
Pradhan Mantri Jan Arogya Yojana (PMJAY) Scheme
Aim: To make path-breaking interventions to address health holistically, in primary, secondary and tertiary care systems
Objective: Prevention + Promotion (Health & Wellness)
Two major initiatives:
- Health and Wellness Centre: Foundation of India’s health system
- 1.5 lakh centres will provide – comprehensive health care, including for non-communicable diseases and maternal and child health services, provide free essential drugs and diagnostic services
- The budget has allocated Rs.1200 crore for this flagship programme
- Contribution of the private sector through CSR and philanthropic institutions in adopting these centres is also envisaged.
- National Health Protection Scheme:
-
- Will cover over 10 crore poor and vulnerable families (approximately 50 crore beneficiaries)
- Coverage of up to ₹5 lakh a family a year will be provided for secondary- and tertiary-care hospitalization (50 crore beneficiaries)
The Concern: The National Sample Survey’s (NSS) health data of 2014 shows that in an estimated total 24.85 crore families in India, there were 5.72 crore cases of hospitalisation. By that calculation, out of the 10-crore families, there would be roughly 2.3 crore hospitalisations in a year. This means that from the Rs 6,556 crore government funds, health insurance agencies on average have only Rs 2,850 to pay per hospitalisation (assuming there are no administrative costs or insurance overheads).
The average out-of-pocket expenditure (OOPE) per hospitalisation is much higher — around Rs 15,244 as per NSS 2014 data, which amounts to Rs 19,500 in 2019-20 assuming a 5 per cent annual inflation. The PMJAY’s budgetary provisions for insurance agencies will barely cover 15 per cent of this expenditure.
Ayushmaan Bharat can be a Game Changer only if:
- Collaboration is the key: The Central government collaborates successfully with State governments and the industry, and focusses aggressively on the operational and implementation aspect of these initiatives. Government and industry should develop partnerships with the focus on improving the coverage and providing access to quality healthcare services to the people.
- Capacity building of the existing resources: Increased capacity-building of the resources at hand during policy formulation.
- Technology: Strong emphasis on the adoption of technology by the entire healthcare ecosystem to provide accessible and affordable patient care to the last mile of the country.
- Role of States: State ownership and commitment of them is critical as the states are expected to agree for 40 per cent share under the NHPS (Health: State subject). Also, absorptive capacity of States needs to be increased.
- Clarity on the Services being provided: More clarity on the kind of services that will be provided by government health facilities and for which conditions patients will have to use private parties and what mechanisms are being thought of.
- Price matters: Establishment of uniform pricing systems for various health interventions, including diagnostics and medicines, and making them transparent by displaying them in hospital premises.
- Community Engagement: Continuum of care system needs to be established by linking institutions or hospitals, with health centres and the community. Community engagement is thus crucial in planning and implementation of the programme and in ensuring that the health and wellness centres and the primary health centres are responsive to the needs of the community.
- Special Unit to measure success, course correct: For effective implementation, an independent body or unit may be set up within the Ministry of Health & Family Welfare to plan, coordinate, and provide technical backstopping to states, including in capacity building and development of standards and guidelines for the programme. Such a unit will ensure uniform and systematic approach to programme implementation across the country.
Some concerns and Way Ahead
Poor public health spending: Government aims to increase public health spending to 5% of GDP. However, current health spending is only 1.15-1.5% of GDP. To reach its target, the government should increase funding for health by 20-25% every year for the next five years or more.
Poor allocation in Interim Budget: The total allocation to healthcare is ₹61,398 crore (an increase of ₹7,000 crore from the previous Budget). However, there is no net increase since the total amount is 2.2% of the Budget, the same as the previous Budget. The increase roughly equates the ₹6,400 crore allocated for implementation of the Ayushman Bharat-Pradhan Mantri Jan Arogya Yojana (PMJAY). The modest increase in budgetary allocations in health should have been prioritised towards improving the worn-out public sector district hospitals, community health centres, primary health centres and sub-centres in under-served areas.
Per capita spending on health: Public per capita expenditure on health increased from ₹621 in 2009-10 to ₹1,112 in 2015-16. Per capita spending on health for 2018 is approx. ₹1,500. Therefore, despite the doubling of per capita expenditure on health over six years, the public spending figure is still abysmal.
Strengthening of the country’s primary healthcare system taken a backseat: Allocation under the National Rural Health Mission (NRHM) — which provides funds for rural primary healthcare — has been reduced in real terms (accounting for inflation). Its share in the health component of the budget has declined steeply over the past four years — from 52 per cent in 2015-16 to 41 per cent this year. Within the NRHM, there have been budget cuts for reproductive and child healthcare projects and maintenance of rural healthcare infrastructure.
Ranking on the basis of Per capita Budget expenditure on health: It is among the lowest in the world. It is important to note that U.S.’s health expenditure is 18% of GDP, while India’s is still under 1.5%. In U.S. allocation for healthcare is 23.5% of the budget and per capita spending on health in the Budget is $3,150. In India, allocation for healthcare is merely 2.2% of the Budget and per capita spending on health in the budget in India is approx $30. There is $4,000-$5,000 per capita spending in OECD countries.
High out-of-pocket expenditure: Out-of-pocket expenditure in India is at a massive 67%. Although, the ₹6,400 crore allocation to Ayushman Bharat-PMJAY in the Interim Budget will help reduce out-of-pocket expenditure on health.
Note:
PM-JAY app: The app has been introduced within just four months since the launch of the scheme and is aimed at helping users get easy access to information on the scheme, check eligibility, find hospitals nearby and get assisted help.
National Health Authority (NHA): Aims to effectively implement PM-JAY. The National Health Authority with a stronger mandate would be able to prevent, detect and control frauds, abuse and redress grievances, thus resulting in the reduction of leakages.
National Health Stack (NHS): A national electronic registry usable by both the Centre and the States across public and private sectors.
- One of the components of the proposed project is to store every Indian’s Personal Health Records (PHRs). This will involve medical history, medication and allergies, immunisation status, laboratory test results, radiology images, vital signs, personal stats such as age and weight, demographics, and billing information, and use of multiple health applications.
- Various layers of the National Health Stack will seamlessly link to support national health electronic registries, coverage and claims platform, a federated personal health records framework, a national health analytics platform, as well as other horizontal components.
- The stack will embrace health management systems of public health programmes and socio-demographic data systems.
- The population level base of such an IT system would be individual health records logged through the Health and Wellness Centres in rural areas, and corresponding primary health care in urban areas.
- The National Health Stack rests on the JAM trinity of Jan Dhan accounts, Aadhaar, and mobile numbers.
The new Digital Information Security in HealthCare Act (DISHA):
- It makes any breach punishable with up to five years’ imprisonment and a fine of Rs. 5 lakhs.
- It redefines personal information of the patients. It adds, “use of narcotic or psychotropic substances, consumption of alcohol, human immunodeficiency virus status, sexually transmitted infections treatment, and abortion” related information of the patient to the list of sensitive information.
- DISHA also defines a ‘clinical establishment’ as well as the term ‘entity’ clearly and unambiguously to include individuals, trusts, private and public establishments, hospitals, diagnostic centres, pathological laboratories, radiology laboratories, etc.
- It also accords great significance to “informed consent” of individuals and emphasises on obtaining explicit consent before transfer and use of digital health data.
₹250 crore has been allocated for setting up health and wellness centres under the National Urban Health Mission. Under the National Rural Health Mission, ₹1,350 crore has been allocated for the same.
Nearly 1.5 lakh health and wellness centres would be set up under Ayushman Bharat.
The non-communicable diseases programme of the National Programme for Prevention and Control of Cancer, Diabetes, Cardiovascular Diseases and Strokehas been allocated ₹175 crore, from ₹275 crore.
Allocation to the National Tobacco Control Programme and Drug De-addiction Programme is only ₹65 crore, a decrease of ₹2 crore.
Must Read:
- Lessons from Kerala : Transforming Primary Care
- Regulating Private Hospitals
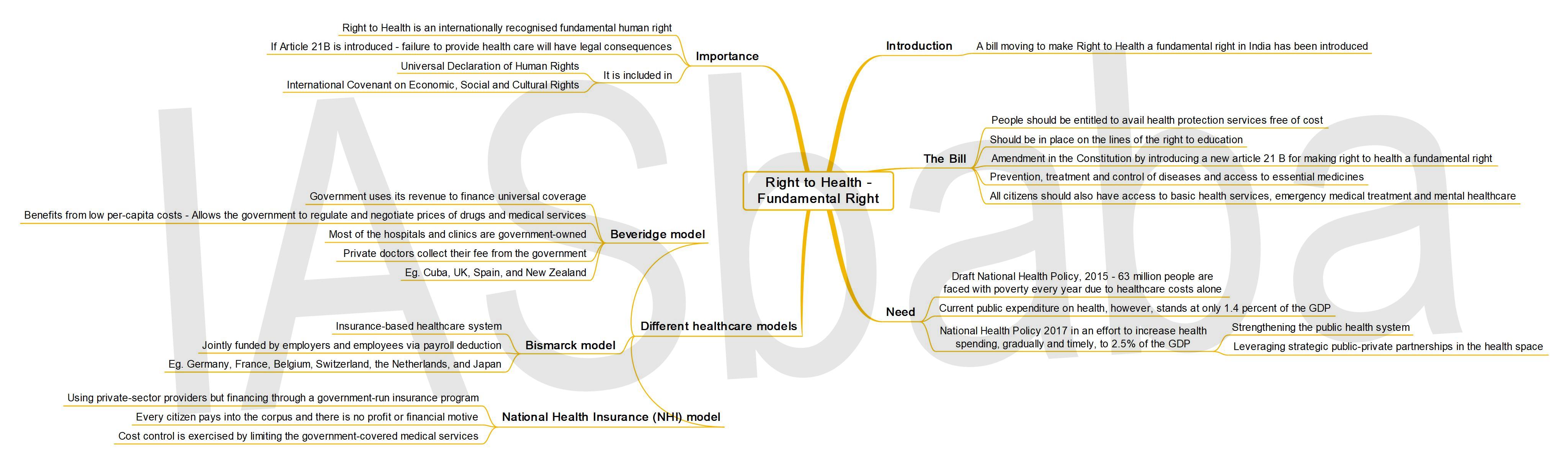
- Right to health – A Fundamental Right
Connecting the Dots:
- What do you understand by universal health coverage? Explain the measures taken by the government to achieve universal health coverage in India.
- India is on the verge of facing an explosion of health epidemic in terms of NCDs if not controlled. Analyse the ways to improve India’s health profile.
- Although the private sector can play a constructive role in the provisioning healthcare services, the overall health policy discourse must retain the ‘public good’ character of the health sector. Comment.
- Ayushman Bharat is one of the most ambitious health schemes ever launched in India. What can be the key challenges in proper implementation of this scheme?



{kind=link}