Effect of policies and politics of developed and developing countries on India’s interests, Indian diaspora.
Issues relating to development and management of Social Sector/Services relating to Health.
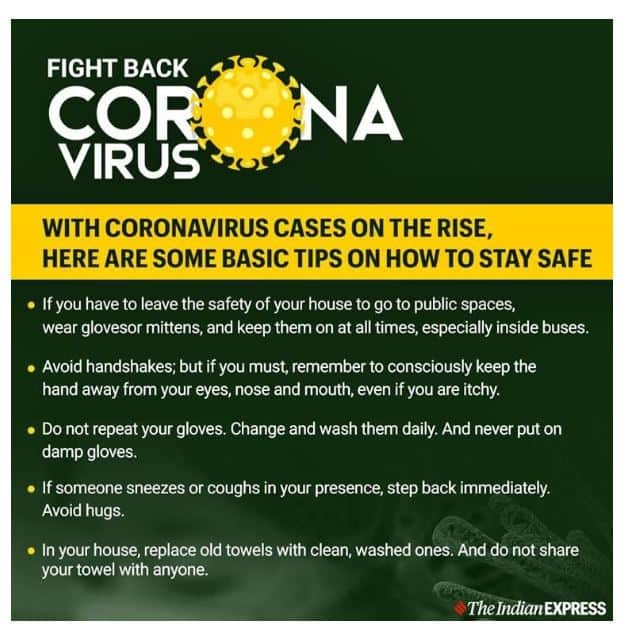
What is Coronavirus?
Coronaviruses are a large family of viruses which cause a range of diseases from the common cold to more severe ones like Severe Acute Respiratory Syndrome (SARS).
Coronavirus versus the flu: What’s the difference?
Both COVID-19 and flu are viral-borne infections which primarily spread through human-to-human contact, such as by means of coughing, respiratory droplets and phlegm.
The coronavirus and flu virus belong to different families. While the flu virus spreads through aerosol, it remains suspended in the air and the other person tends to catch it. On the other hand, coronavirus is more likely to spread by contact, for instance, touching the same surface
According to WHO, COVID-19 and the flu are both contagious viruses that cause respiratory illness and lead to symptoms such as nausea, shortness of breath, chest congestion, rise in temperature and if it gets difficult to contain, lead to pneumonia. While symptoms can appear anywhere between three to four days for flu, it takes two to 14 days for coronavirus symptoms to appear.
While symptoms for both include cough and cold, fever, runny nose, the only difference seen is when the sample is sent for testing. A polymerase chain reaction (PCR) test is done for flu where we test for the RNA (or Ribonucleic acid which is essential for any form of life) of the virus. For both the viruses, different PCR tests are done. Genotype of both the viruses are different. It can be differentiated only by lab tests, while clinically, it is next to impossible.
Flu is seasonal. It takes place every year while no one knows of coronavirus — whether it is seasonal or not, because it’s a new infection
Awareness over COVID 19 – All India Radio (AIR) IAS UPSC
How to handle coronavirus (COVID-19) as a Country?
In India, the National Centre for Disease Control (NCDC), state governments and WHO offices have established plans and procedures to detect and isolate the first cases of COVID-19 as they emerge. The country is working with customs and carriers to enhance health measures. The state governments have to identify, isolate and contain cases. Fifteen government laboratories have the approval to test for COVID-19 and another 19 are being prepared to test samples to ensure an adequate geographical spread across the country.
Whenever the country faces public health emergencies, it is better to overreact and then scale back if necessary rather than under-react and then act too late. Here are the most important aspects of such planning required for the country.
A robust surveillance system is important as the backbone for planning any action. The Centres for Disease Control in the United States (US) operates on five times higher budget than that of NCDC in India which caters to four times larger population. It is time the government prioritised the strengthening of the surveillance systems.
The quantum of research and its progress regarding SARS-CoV-2 is unprecedented in the history of science and public health. In the coming days, more than 100 research projects will provide significant insights into which tests and drugs to use and finding a safe and effective vaccine. As a result, a vaccine against Covid-19 might be realised soon with the first set candidate vaccines entering phase 1 trials by next few weeks. In a recent article published in Vaccine, Matthew McKay and others report that no mutations are present in the SARS-CoV-2 and hence, it is possible to design a vaccine by immune targeting. Scientists at Novavax have announced that their recombinant protein nanoparticle technology platform can be used to generate antigens derived from the coronavirus spike protein.
The therapy currently consists of supportive care. No drug has yet been approved to treat coronavirus infections in humans. If everything goes well, new drugs can be developed and deployed by 2021. These drugs are targeted for other strains of virus that have not yet been identified in causing outbreaks. For example, there are drugs tested to act on a spike-shaped protein on the surface of these viruses. However, we need to be cautious as all the ongoing studies are in nascent stages and have to go through several phases before they are available for human use. However, several of the drugs already approved for other antiviral indications are being tested and are in advanced stages.
Intravenous hyperimmune globulin, by concentrating the pathogen-specific antibodies from plasma collected from recovered patients, can be helpful in reducing the severity of illness. Some research groups in China have found antibodies can act on the spike proteins, preventing coronaviruses from attacking human cells.
As we move forward, the drugs, diagnostics and vaccines can be evaluated in scientifically and ethically sound studies with the evolving phases of outbreak. The governments need to step up investments and actions to conduct research in tackling COVID-19.
Note: World Health Organization (WHO) gave an official name to the disease caused by the novel coronavirus. The disease will be called “COVID-19”; the “CO” stands for coronavirus, “VI” for virus and “D” for disease. The coronavirus itself is called “nCoV-2019”.